What is a Trali

Robert Spencer
Published May 27, 2026
Transfusion-related acute lung injury (TRALI) is a rare but potentially fatal complication of blood product transfusion. The epidemiology, pathogenesis, risk factors, clinical features, management, and prevention strategies for TRALI are presented here.
What causes a TRALI?
The etiology of TRALI may be attributable to the presence of anti-HLA and/ or anti-granulocyte antibodies in the plasma of multiparous females or donors who have received previous transfusions. TRALI recipients have no specific demographics such as age, gender, or previous transfusion history.
What is the treatment for TRALI?
Treatment / Management Immediate management of TRALI is to stop the transfusion and notify the blood bank to screen the donor unit for antileukocyte antibodies, anti-HLA or anti-neutrophil-specific antibodies. [5] Supportive measures must be taken to improve oxygenation.
What are TRALI antibodies?
However, we do know that units of plasma or platelets that have caused a TRALI reaction in a transfusion recipient often contain antibodies to human leukocyte antigens (HLA). These antibodies are known as HLA antibodies and are on the white blood cell (leukocyte) surfaces.What signs or symptoms are potential indications of TRALI?
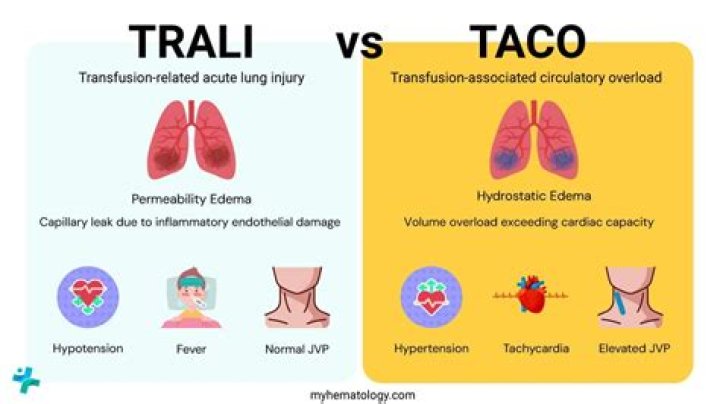
Symptoms of TRALI typically develop during or within 6 hours of a transfusion. Patients present with rapid onset of dyspnea and tachypnea, with an SpO2 < 90% on room air. There may be associated fever, cyanosis and hypotension.
Can you recover from TRALI?
TRALI (transfusion-related acute lung injury) Symptoms include tachypnea, dyspnea, hypotension and fever; hypoxia may be profound and the chest radiograph demonstrates diffuse pulmonary infiltrates. Patients usually recover within 24 hours with supportive care.
How often does TRALI occur?
TRALI is an uncommon syndrome, that is due to the presence of leukocyte antibodies in transfused plasma. It is believed to occur in approximately one in every 5000 transfusions.
How is TRALI diagnosed?
To diagnose TRALI, physical exam, chest x-ray, and arterial blood gas studies are recommended. In distinguishing TRALI from TACO, an echocardiogram may be useful in determining whether the observed pulmonary edema is of cardiogenic origin.What is the mortality rate of TRALI?
Among immediate transfusion reactions, TRALI is singular in its mortality rate. Only hemolytic transfusion reactions due to ABO incompatibility are comparable. The reported fatality rate is 5–24%. The most widely cited figure is 5–10% [3].
Is it bad to have HLA antibodies?HLA antibodies are not harmful to the person who made them. Your HLA antibodies pose absolutely no risk to you. However, if transfused to another person HLA antibodies can cause a rare but very serious complication in the transfusion recipients known as Transfusion-Related Acute Lung Injury (TRALI).
Article first time published onWho is at risk for TRALI?
Critically ill patients may be at greater risk for TRALI because of underlying severe illness, and a retrospective study estimated the risk of TRALI and possible TRALI to be 1 in 1271 units transfused to patients in intensive care units (52).
Is TRALI a type of ARDS?
2) TRALI has been separated into two types: TRALI type I (without an acute respiratory distress syndrome (ARDS) risk factor) and TRALI type II (with an ARDS risk factor or with mild preexisting ARDS).
What are risk factors for TRALI?
Conclusions: The risk factors for TRALI in this study included Number of transfusions and FFP units were positively correlated with TRALI. Age, female sex, tobacco use, chronic alcohol abuse, positive fluid balance, shock before transfusion, ASA score and mechanical ventilation may be potential risk factors for TRALI.
Is TRALI immune mediated?
About two thirds of TRALI cases are thought to be immune-mediated. Both Human Leucocyte Antibodies (HLA Class I and II) and Human Neutrophil Antibodies (HNA) are involved in TRALI.
How can TRALI be prevented?
- Screening of all donors for anti-neutrophil or anti-HLA antibodies. …
- Use of pre-storage leukoreduced blood. …
- Appropriate utilization of blood products.
What is the difference between Taco and TRALI?
Diagnostically, it remains very challenging to distinguish TACO and TRALI from underlying causes of lung injury and/or fluid overload as well as from each other. TACO is characterized by pulmonary hydrostatic (cardiogenic) edema, whereas TRALI presents as pulmonary permeability edema (noncardiogenic).
What does taco stand for in blood transfusion?
IHN/ISBT haemovigilance working party/AABB. Web_March 2019. Transfusion-associated circulatory overload (TACO) Definition (2018) International Society of Blood Transfusion.
What causes taco?
Transfusion-associated circulatory overload (TACO), also known as transfusion-induced cardiogenic pulmonary edema, is caused by an inability of the recipient to compensate for the transfused volume. Despite being underreported, TACO is among the most common transfusion reactions.
Why does a blood transfusion cause ARDS?
Similarly, Gong and colleagues [9], in an analysis of 700 patients, noted that transfusion was significantly associated with the evolution of ARDS. Mechanistically, some speculate that pRBC transfusion could promote ARDS because transfusion activates pro-inflammatory cascades [11,12].
Can IVIG cause TRALI?
IVIG is a pooled plasma derivative commonly used in the outpatient setting. Respiratory complications of IVIG infusion have typically been attributed to volume overload or allergic and vasomotor reactions. TRALI has never been documented to occur after IVIG infusion.
Which type of HNA have clinical significant causing TRALI?
HNA-3a antibodies are the most frequently detected of the HNA antibodies in TRALI cases, seen in up to 85% of cases7 ; can induce TRALI in the context of minimal residual plasma volume, such as from red cell transfusion; and account for a disproportionate share of TRALI fatalities compared with other mediators.
What does it mean to test positive for HLA?
A positive test means HLA-B27 is present. It suggests a greater-than-average risk for developing or having certain autoimmune disorders. An autoimmune disorder is a condition that occurs when the immune system mistakenly attacks and destroys healthy body tissue.
What do my HLA results mean?
Specific HLA genes or antigens are identified during HLA testing to ensure solid organ or hematopoietic stem cell transplant compatibility. The typing result of the recipient is compared to those of the potential donor. Results indicate how many antigens match and how many antigen mismatches are present. “
How did I get HLA antibodies?
A: Anti-HLA antibodies are formed by the immune system when you are exposed to proteins that appear similar to tissue types. This most commonly occurs in the setting of previous transplantation, pregnancy, or blood transfusion. Occasionally the cause of anti-HLA antibody formation is not known.
Can blood transfusion cause fluid in lungs?
Objective: Pulmonary edema is an under-recognized and potentially serious complication of blood transfusion. Distinct mechanisms include adverse immune reactions and circulatory overload.
What is post transfusion purpura?
Post-transfusion purpura (PTP) is a rare yet serious disease characterized by severe thrombocytopenia occurring after a blood transfusion. It is caused by alloimmunization against platelet antigens, anti-HPA-1a being the most frequent antibody.
How do you make cryoprecipitate?
To create cryoprecipitate, fresh frozen plasma thawed to 1–6 °C is then centrifuged and the precipitate is collected. The precipitate is resuspended in a small amount of residual plasma (generally 10–15 mL) and is then re-frozen for storage.