How long can an IO be used

Robert Spencer
Published Apr 02, 2026
The IO site can be used for 24 hours and should be removed as soon as intravenous access has been gained. Prolonged use of an IO site, lasting longer than 24 hours, is associated with osteomyelitis (an infection in the bone).
How long can an intraosseous needle remain in situ?
The intraosseous needle may remain in situ for 72 to 96 hours, but it is best removed within 6 to 12 hours, as soon as an alternative site of intravascular access has been established. The intraosseous route provides fast and reliable vascular access in emergency medical situations.
When can an IO be used?
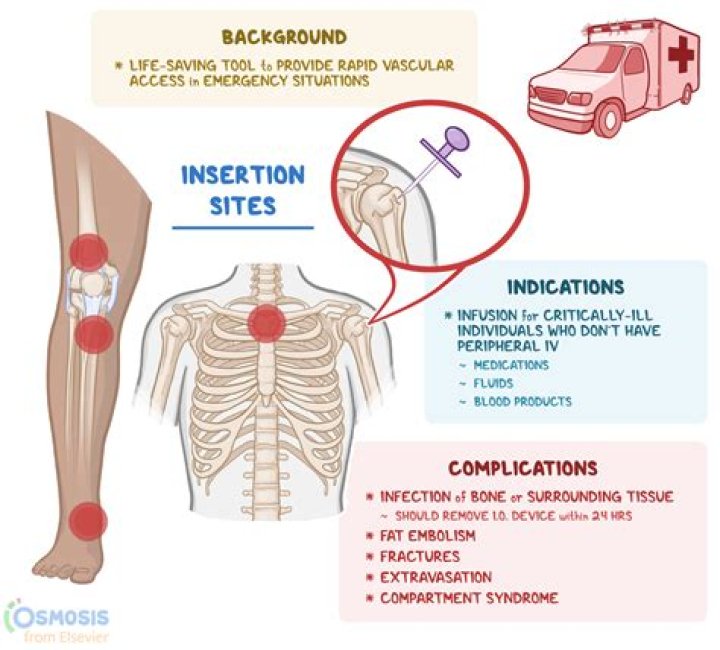
IO access has been used in medical emergencies requiring immediate access when peripheral IV access is either not possible or time-prohibiting, such as cardiac arrest, status epilepticus, shock, trauma, and burns[2]. There is mounting evidence supporting the continued use of IO lines both in-hospital and pre-hospital.
When should an IO be removed?
IO access is meant to be temporary venous access. IO devices should be removed as soon as other venous access is established or within 24 hours after insertion.When can IO access not be used?
In a general manner, IO access should not be used in severe genetic or acquired bone diseases, imperfect osteogenesis, osteoporosis and osteomyelitis [17].
How bad does an IO hurt?
The procedure is both safe and effective in children and adults. IO access can be extremely painful. However, the patient’s pain level can be reduced to a bearable level by injecting 2% preservative-free lidocaine through a special port before starting the infusion.
Is Io considered a central line?
IO techniques have fewer serious complications than central lines, and they can be performed much faster than central or peripheral lines when vascular collapse is present. IO insertion is recognized to be both safe and effective in all children and adults.
Can you give blood through IO?
Any intravenous fluid, blood products or routine resuscitation drugs can be administered through the IO route. Complications for short term use are relatively rare compared to the advantages for a child who needs rapid administration of blood or fluid.Why would someone need an IO?
Intraosseous access is indicated in emergent situations, such as when a person experiences some type of major trauma like shock, cardiac arrest, severe dehydration, or severe gastrointestinal hemorrhage. IO access can provide the quickest way to rapidly infuse needed medications and fluids in an emergency situation.
How do I cancel my io?- Remove extension set from needle hub and attach a 5 or 10mL sterile syringe with standard luer lock to act as a handle and cap the open IO port.
- Grasp syringe and continuously rotated clockwise while gently pulling until the needle is removed.
Can you Io a neonate?
Gaining vascular access in a neonate during cardiopulmonary resuscitation is crucial and challenging. Intraosseous (IO) access can offer a fast and reliable method for achieving emergency access for fluids and drugs when venous access fails in a critically ill child.
Where do you put IO on a neonate?
Sites. The entry point is a few centimetres below the tibial tuberosity at the centre of the flat antero-medial surface. The needle is directed caudal away from the upper tibial epiphysis in the line of the shaft.
When should IO access be attempted before vascular?
Indications. IO access is the recommended technique for circulatory access in cardiac arrest. In decompensated shock IO access should be established if vascular access is not rapidly achieved (if other attempts at venous access fail, or if they will take longer than ninety seconds to carry out.)
Is IO better than IV?
Intraosseous (IO) parenteral access is relatively fast and easy to obtain, whereas intravenous (IV) access can be difficult. IO access is currently recommended as an option for patients with out-of-hospital cardiac arrest (OHCA) when IV access cannot be immediately obtained.
Is IO quicker than IV?
An IO is a quick way to get vascular access in a code, faster than an IV and with greater first-attempt success.
How fast can you run fluids through an intraosseous cannula?
The maximum rate of administration through the IO needle was reportedly equivalent to a 21 G peripheral cannula [23]. The flow rates of an intravenous cannula are typically in the range of 200 (16 G peripheral cannula) to 20 ml/min (24 G peripheral cannula) [30].
Can glucose be given io?
Intraosseous infusion of hypertonic glucose and dopamine is an effective route by which to administer these medications and is potentially useful in emergency situations in which intravascular access is delayed.
Can you start an IV in bone?
The bone drill. … A bone drill is used when a traditional IV cannot be secured on a patient. It could be because the patient is dehydrated, diabetic or under extreme trauma, Shubert said. The bone drill can be used to quickly insert an intraosseous needle directly into the bone to dispense fluids, medications or sugar.
How much lidocaine does it take to flush an IO?
9%) flush. Consider a lower flush volume in younger children and infants. o The initial guideline dose for children and adults is 0.5 mg/kg. This is presented as the volume of 2% preservative-free lidocaine to be given IO.
What labs are inaccurate from Io?
Labs drawn via IO There is not good correlation with Sodium, Potassium, CO2, and calcium levels.
Can nurses place IO lines?
RN’s, physicians or EMT-P’s may insert an IO device after they have completed instruction with clinical supervision. An order must be received to by a physician for a RN or EMT-P to insert an IO. 3. … RN must place the IV fluid bag on either a pressure bag or use an IV pump for infusion.
Can you use a rapid infuser with an IO?
IO access is one of the quickest ways to establish vascular access for the rapid infusion of fluids, drugs, and blood products in an emergency. In adults and pediatrics after 2 peripheral IV attempts, IO is the next-line modality.
Can Propofol be given io?
Two IO doses of propofol (1 mg/kg) were administered during the direct laryngoscopy to achieve a deeper plane of anesthesia. After completion of the airway examination, which required 15 min, the infant was transported to the pediatric ICU with the IO needle in place.
What drugs can be given io?
While all resuscitation drugs can be given by the IO route, administration of ceftriaxone, chloramphenicol, phenytoin, tobramycin, and vancomycin may result in lower peak serum concentrations. The most common adverse effect seen with IO use, extravasation, has been reported in 12% of patients.
How do you confirm intraosseous needle placement?
A properly placed IO line must be through the cortex of the bone and situated within the marrow cavity. Standard methods for confirmation of IO placement include aspiration of bone marrow, firm placement of the IO needle into the bone, and no evidence of extravasation.
What is a intraosseous catheter?
Intraosseous (i.o.) catheterization is frequently used in veterinary medicine to provide fluids and other medications when intravenous (i.v.) access is not available or difficult to obtain. This may occur as a result of hypovolemia during illness or simply small peripheral vein size.
What size is the yellow IO needle?
EZ-IO® IO-IV devices may be inserted with a power driver (drill) or manually. The 25 mm (blue hub) and 15 mm (pink hub) needles may be inserted manually. The 45 mm (yellow hub) requires a power drill for insertion and does not come with a manual driver.
What site is the first choice for intraosseous infusion?
The proximal tibia, humeral head, and sternum are the preferred sites in adults. The distal femur, proximal tibia, and distal tibia are preferred sites for infants and neonates.
Does IO placement yield blood return?
There are already multiple methods for confirming IO placement, including return of bone marrow, visualization of blood in the stylet, firm placement of the needle in the bone, and the ability to smoothly deliver a fluid flush.
Which condition in a child should IO access most likely be attempted before vascular access?
I/O before vascular access – for cardiac arrest. Labs – lethargy, Polyuria, onset rapid, deep, labored breathing – assess blood glucose. Motor vehicle accident, immediate intervention for decreased level of consciousness.
Can adrenaline be given io?
Background: Adrenaline is an important component in the resuscitation of individuals experiencing out-of-hospital cardiac arrest (OHCA). The 2018 Advanced Cardiac Life Support (ACLS) algorithm gives the option of either intravenous (IV) or intraosseous (IO) routes for adrenaline administration during cardiac arrest.