How is acute GVHD treated

Emily Dawson
Published Feb 12, 2026
The main treatment is steroids, which generally work well. Your doctor might also treat you with other drugs to suppress your immune system and so reduce the GvHD. Light therapy with extracorporeal photophoresis can also help.
Does acute GVHD go away?
GVHD usually goes away a year or so after the transplant, when your body starts to make its own white blood cells from the donor cells. But some people have to manage it for many years.
What is GVHD how is it managed?
Management of GVHD is challenging. Immuno-suppression with corticosteroids forms the basis of first-line therapy in both acute and chronic GVHD, producing sustained responses in less than 50% of patients with aGVHD and 40–50% of patients with cGVHD depending on initial disease severity.
How long does acute GVHD last?
ECP for acute GvHD responds quite quickly, whereas ECP for chronic GvHD can take six months or more before any improvement. In some cases, treatment can last 12–18 months or longer.How is GVHD diagnosis?
The diagnosis of acute GVHD can be made readily on clinical grounds in the patient who presents with a classic maculopapular rash, abdominal cramps with diarrhea, and a rising serum bilirubin concentration within two to three weeks following hematopoietic cell transplantation (HCT).
What is GVHD stage4?
Grade 4 is very severe GvHD. Your skin has blistered and may have broken down in places. Your skin may be yellow (jaundiced) because your liver is not working properly. You have severe diarrhoea.
What is ECP treatment for GVHD?
Extracorporeal photopheresis (ECP) is a cutting-edge, nonsurgical procedure to treat graft-versus-host disease (GVHD), a complication of bone marrow and stem cell transplants and other autoimmune disorders in children. ECP is also used to treat solid organ transplant rejection.
What is the difference between acute and chronic GVHD?
By definition, acute GVHD is any reaction that occurs within the first 100 days after transplant, and chronic GVHD is reactions that occur after 100 days.How do you treat GVHD?
The skin is the most common part of the body affected by chronic GvHD. The treatment includes keeping your skin clean and moisturising regularly. You should use unperfumed soaps and moisturising creams. Your doctor prescribes steroid creams or a cream called tacrolimus if the skin problems are just in small areas.
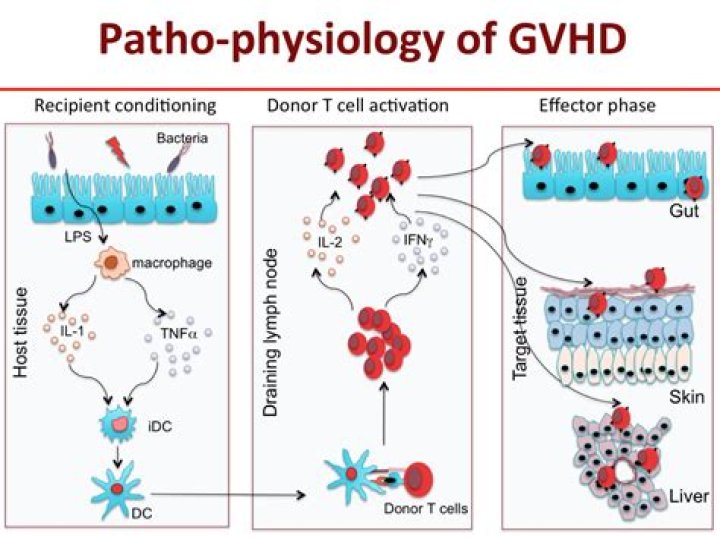
What is acute GVHD?Acute graft-versus-host-disease (acute GVHD) occurs when lymphocytes from another person are able to survive and proliferate in a patient; it is one of the most serious complications of allogeneic bone marrow transplantation (BMT).
Article first time published onHow often is GVHD fatal?
Chronic GVHD affects approximately 30% to 80% of patients surviving 6 months or longer after stem cell transplantation and is the leading cause of nonrelapse deaths occurring more than 2 years after transplantation.
How do you prevent GVHD?
GvHD can develop when the donor and the person receiving donor cells have a different tissue type. So your transplant specialist will make sure your donor is as closely matched to you as possible. This is called tissue typing and helps reduce your risk of GvHD.
What does GVHD of the skin look like?
Chronic GVHD of the skin happens when the donor’s cells attack your skin. It is the most common type of chronic GVHD. Chronic GVHD of the skin can cause color changes (red, pink, purple, brown or white), thinning or thickening, hardening, rashes, scaly areas, bumps, sores or blisters (small pockets of fluid).
What causes GVHD?
GVHD may occur after a bone marrow, or stem cell, transplant in which someone receives bone marrow tissue or cells from a donor. This type of transplant is called allogeneic. The new, transplanted cells regard the recipient’s body as foreign. When this happens, the cells attack the recipient’s body.
Is GvHD a good thing?
In some cases GvHD is serious, and can even life threatening. But having mild GvHD can be a good thing. As well as attacking your body cells, the donor T cells will also attack any remaining cancer cells. Doctors call this the graft versus disease effect.
How much does extracorporeal photopheresis cost?
The time for ECP was 117 min (median, range: 91-164 min) using CELLEX and 161 min (median; range: 140-210) using the UVAR-XTS machine. Total costs of each ECP procedure were $3420.50. There is a considerable time commitment of the patient and the clinical staff when employing ECP to treat GVHD.
What is the life ECP?
ECP is also called extracorporeal photopheresis. ECP is a treatment for GvHD which is designed to destroy the T cells and white blood cells which cause the GvHD. The process is very similar to how stem cells are collected for donation.
What are the stages of GVHD?
StageSkinGI/Gut (stool output per day)cAdult1Maculopapular rash <25% BSA500–999 mLd or 3–4 episodes/day2Maculopapular rash 25%–50% BSA1,000–1,500 mL or 5–7 episodes/day3Maculopapular rash >50% BSA>1,500 mL or >7 episodes/day
How serious is GVHD?
GVHD is a serious and potentially life-threatening condition in which the donor cells attack the recipient’s healthy cells, causing a range of medical problems.
What is the average life expectancy after bone marrow transplant?
Some 62% of BMT patients survived at least 365 days, and of those surviving 365 days, 89% survived at least another 365 days. Of the patients who survived 6 years post-BMT, 98.5% survived at least another year.
Can GVHD cause death?
Chronic graft-v-host disease (chronic GVHD) is a frequent cause of late morbidity and death after bone marrow transplantation (BMT). The actuarial survival after onset of chronic GVHD in 85 patients was 42% (95%Cl = 29%, 54%) at 10 years.
What is sclerotic GVHD?
Sclerotic GVHD displays as dermatological lesions including thickening of the skin or as fascial lesions such as limited ranges of motion in joints, resulting in wall chest compression and impairment of wound healing.
Which is worse acute or chronic GVHD?
GVHD is a major determinant of the long-term QOL of survivors. The adverse effects of acute GVHD are detectable with the TOI at 6 months post transplantation after which development of chronic GVHD is the most strongly correlated with worse QOL.
How do I heal my gut after GVHD?
Medicines, like topical steroids that you swallow, can ease symptoms. These coat your stomach and intestines without affecting the rest of your body. Examples are beclomethasone in corn oil and budesonide pills. Most people with this type of chronic GVHD will also need medicines that treat the entire body.
How do you treat GVHD Diarrhea?
GvHD of the gut might cause sickness or diarrhoea. The main treatment is steroids, which generally work well. Your doctor might also treat you with other drugs to suppress your immune system and so reduce the GvHD. Light therapy with extracorporeal photophoresis can also help.
How common is acute GVHD?
Acute GVHD can occur in up to 50% of patients receiving hematopoietic stem cell transplantation (HCT) from a human leukocyte antigen (HLA)-matched sibling [5] [6]. The occurrence is typically higher in unmatched donors. The incidence of chronic GVHD ranges from 6% to 80% [7].
What does GVHD mean in medical terms?
Graft-versus-host disease (GVHD) is a life-threatening complication that can occur after certain stem cell or bone marrow transplants.
What is graft failure?
Graft failure is a serious complication of allogeneic hematopoietic stem cell transplantation (allo-HSCT) defined as either lack of initial engraftment of donor cells (primary graft failure) or loss of donor cells after initial engraftment (secondary graft failure).
What are the three requirements for GVHD?
Fifty years ago Billingham formulated three requirements for the development of GVHD: the graft must contain immunologically competent cells; the recipient must express tissue antigens that are not present in the transplant donor; and the recipient must be incapable of mounting an effective response to eliminate the …
Who is at risk for GVHD?
Patients who have an increased risk of developing cGvHD are: Those who’ve received stem cells/bone marrow from an HLA (human leukocyte antigen) mismatched related donor or from an HLA matched unrelated donor. Patients who may have already experienced acute GvHD. Older transplant recipients.
How do you prevent grafts?
- Reducing the risk from tissue type. …
- Suppressing the immune system. …
- Removal of T cells (T cell depletion) …
- Inhibition of T cell proliferation. …
- Reduction intensity of conditioning processes. …
- Environment. …
- Sunlight. …
- Host antigen-presenting cells (APCs)