How do you push RSI drugs

Emily Dawson
Published Feb 24, 2026
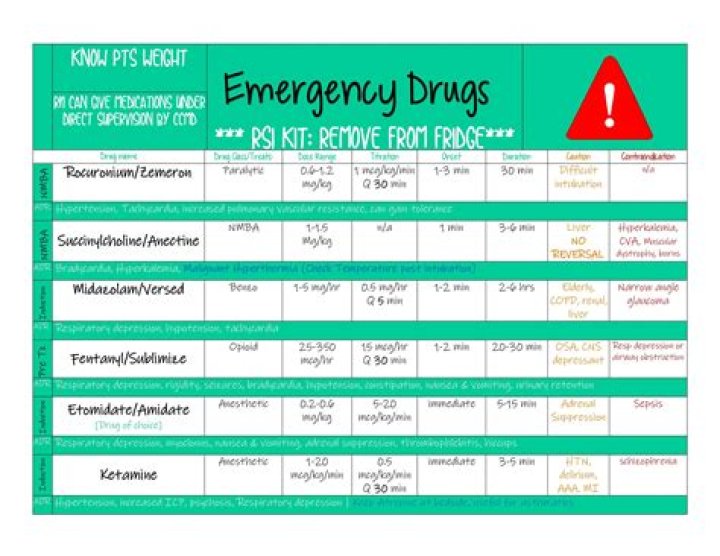
Use IV access on the opposite side of the blood pressure cuff. Always follow RSI drugs with analgesia first after the tube is secured. Give the RSI drugs rapidly, fast IV push, sedative first, then the paralysing agent followed by a large flush or fluid bolus.
How fast can succinylcholine be pushed?
For small doses, may dilute to a concentration of 1 to 2 mg/mL in a compatible intravenous solution (5% Dextrose Injection or 0.9% Sodium Chloride Injection). Administer via IV push over 10 to 30 seconds. Monitor heart rate and blood pressure carefully during administration.
What happens when you push etomidate too fast?
Although uncommon, overdosage may occur from rapid or repeated injections. A decrease in blood pressure may follow rapid injection. No adverse cardiovascular or respiratory effects due to etomidate overdose have been reported.
Can Nurses push RSI drugs?
The Nevada State Board of Nursing finds that it is within the scope of practice of a registered nurse (RN) to administer IV anesthetic agents for the purpose of Rapid Sequence Intubation (RSI) if the RN is in the presence of a legally authorized practitioner credentialed in emergency airway management and …What order do you give RSI drugs?
- Plan.
- Preparation (drugs, equipment, people, place)
- Protect the cervical spine.
- Positioning (some do this after paralysis and induction)
- Preoxygenation.
- Pretreatment (optional; e.g. atropine, fentanyl and lignocaine)
- Paralysis and Induction.
- Placement with proof.
How long does etomidate last for RSI?
Because of its positive hemodynamic profile, etomidate has become the sedative of choice for RSI. Etomidate is an imidazole derivative dosed at 0.3 mg/kg IV; the time of onset is 15-30 seconds, and the duration of action is approximately 3-12 minutes.
Do you push succ or etomidate first?
It is usually not of concern when used in paralytic RSI since the rapid administration of Succinylcholine quickly paralyzes the masseter muscles. Etomidate, when used in paralytic RSI, is pushed as rapidly as possible and is immediately followed by the neuromuscular blocking agent.
Do you reverse succinylcholine?
Sugammadex can reverse profound blockade and can be given for immediate reversal and its use would avoid the potentially serious adverse effects of the currently used agent, succinylcholine. Also, sugammadex can reverse NMB more quickly and predictably than existing agents.What is the onset of action for succinylcholine?
The onset of effect of succinylcholine given intramuscularly is usually observed in about 2 to 3 minutes. Succinylcholine is acidic (pH 3.5) and should not be mixed with alkaline solutions having a pH greater than 8.5 (e.g., barbiturate solutions).
Can nurses administer succinylcholine?The registered nurse (RN) may administer Propofol, Etomidate and neuromuscular blocking agents (only Succinylcholine, Rocuronium and Vecuronium) to the non-intubated patient in a hospital setting for the purpose of rapid sequence intubation when the clinical presentation of impending respiratory failure is imminent.
Article first time published onCan an RN push propofol?
Administration of IV Anesthetic Agents – Exception Registered Nurses, who are competent in the procedure through education and experience, may administer Propofol to intubated, ventilated patients in a critical care setting based on an appropriate medical order.
Can a nurse anesthetist administer propofol?
Propofol is meant to cause deep sedation. … If an anesthesiologist or certified registered nurse anesthetist (CRNA) with ACLS training is present, gives the order, and has the management of the patient’s airway as their sole responsibility, an RN might feel safe pushing propofol.
How fast does etomidate work?
Etomidate is a hypnotic drug without analgesic activity. Intravenous injection of etomidate produces hypnosis characterized by a rapid onset of action, usually within one minute. Duration of hypnosis is dose dependent but relatively brief, usually three to five minutes when an average dose of 0.3 mg/kg is employed.
What is the reversal agent for etomidate?
Calabadion 2 dose-dependently reverses the effects of ketamine and etomidate on electroencephalographic predictors of depth of anesthesia, as well as drug-induced hypotension, and shortens the time to recovery of righting reflex and functional mobility.
Does etomidate increased ICP?
Conclusions: In pediatric patients with severe traumatic brain injury, single-dose etomidate administration resulted in statistically significant reductions in ICP and improvement in cerebral perfusion pressure without significantly altering MAP.
Is etomidate a sedative?
Conclusion: Etomidate is a useful agent for carefully conducted procedural sedation because it provides effective, brief, deep sedation with little hemodynamic compromise. Its safety may be jeopardized by the occurrence of respiratory depression in older patients receiving higher doses.
Is succinylcholine a paralytic?
Succinylcholine has been traditionally used as a first-line paralytic due to its quick onset of action and short half-life. Succinylcholine’s duration of action is 10—15 minutes, whereas the half-life of rocuronium is anywhere from 30—90 minutes, depending on the dose.
Is propofol used for RSI?
When used for RSI, propofol administration was associated with satisfactory intubating conditions that were comparable to those seen with thiopental and etomidate. Blood pressure reductions were seen in both DCC and RSI studies.
Do you give sedative or paralytic first?
It is commonly recommended that the sedative agent be administered before the paralytic agent. However, administration of the paralytic agent first may allow for decreased apnea time and increased first-pass success by shortening the time between the start of RSI drug administration and paralysis.
How will you perform rapid sequence induction?
Rapid sequence induction (RSI) is a method of achieving rapid control of the airway whilst minimising the risk of regurgitation and aspiration of gastric contents. Intravenous induction of anaesthesia, with the application of cricoid pressure, is swiftly followed by the placement of an endotracheal tube (ETT).
How do you give succinylcholine?
Intramuscular Use If necessary, succinylcholine may be given intramuscularly to infants, older children, or adults when a suitable vein is inaccessible. A dose of up to 3 to 4 mg/kg may be given, but not more than 150 mg total dose should be administered by this route.
Is etomidate a paralytic or sedative?
Etomidate is the most commonly used induction agent for rapid sequence intubation. It is a nonbarbiturate-sedative, which depresses central nervous system function by activating gamma-aminobutyric acid (GABA) receptors.
Does etomidate lower seizure threshold?
Conclusions: Etomidate has a distinct advantage over thiopental in producing seizures of adequate duration during ECT and should be used as the first-line measure in augmenting seizures in patients who have very high seizure thresholds.
Is etomidate a benzo?
Etomidate (Amidate) is a carboxylated derivative of imidazole with pharmacological properties that are similar to barbiturates and benzodiazepines.
How long does it take for nimbex to wear off?
When administered during stable opioid/nitrous oxide/oxygen anesthesia, 0.15 mg/kg of NIMBEX produced maximum neuromuscular blockade in about 2 minutes (range: 1.3 to 4.3 minutes) with a clinically effective block (time to 25% recovery) for about 43 minutes (range: 34 to 58 minutes) [see Clinical Studies].
How fast do you give rocuronium?
The recommended initial dose of rocuronium bromide, regardless of anesthetic technique, is 0.6 mg/kg. Neuromuscular block sufficient for intubation (80% block or greater) is attained in a median (range) time of 1 (0.4 to 6) minute(s) and most patients have intubation completed within 2 minutes.
When should you not take Suxamethonium?
Thus, suxamethonium may be used safely in patients with chronic hyperkalemia that is only moderate (i.e., potassium <6.5 mmol/l). In patients with acute hyperkalemia or chronic hyperkalemia that is severe, suxamethonium should be avoided.
Can succinylcholine be reversed with neostigmine?
It is concluded that succinylcholine-induced phase II block can be safely and rapidly antagonized with neostigmine.
How is succinylcholine apnea treated?
Administration of cholinesterase inhibitors, such as neostigmine, is controversial for reversing succinylcholine-related apnea in patients who are pseudocholinesterase deficient. The effects may be transient, possibly followed by intensified neuromuscular blockade.
Is succinylcholine still used?
With the recent introduction of sugammadex in the United States, a drug that can rapidly reverse even large amounts of rocuronium, succinylcholine should no longer be used for endotracheal intubation and its use should be limited to treating acute laryngospasm during episodes of airway obstruction.
Can RN administer etomidate?
It is not within the scope of practice of the registered nurse who is not a qualified anesthesia provider to administer anesthetic agents (such as Propofol,Ketamine, Etomidate, or Fospropofol). These agents should be administered only by persons trained and educated in the administration of general anesthesia.